Carpal tunnel syndrome occurs when the median nerve, which runs from the forearm into the hand, becomes pressed or squeezed at the wrist. The median nerve controls sensations to the palm side of the thumb and fingers (although not the little finger), as well as impulses to some small muscles in the hand that allow the fingers and thumb to move. The carpal tunnel – a narrow, rigid passageway of ligament and bones at the base of the hand – houses the median nerve and tendons. Sometimes, thickening from irritated tendons or other swelling narrows the tunnel and causes the median nerve to be compressed. The result may be pain, weakness, or numbness in the hand and wrist, radiating up the arm. Although painful sensations may indicate other conditions, carpal tunnel syndrome is the most common and widely known of the entrapment neuropathies in which the body’s peripheral nerves are compressed or traumatized.
Symptoms of carpal tunnel syndrome usually start gradually, with frequent burning, tingling, or itching numbness in the palm of the hand and the fingers, especially the thumb and the index and middle fingers. Some carpal tunnel sufferers say their fingers feel useless and swollen, even though little or no swelling is apparent. The symptoms often first appear in one or both hands during the night, since many people sleep with flexed wrists. A person with carpal tunnel syndrome may wake up feeling the need to “shake out” the hand or wrist. As symptoms worsen, people might feel tingling during the day. Decreased grip strength may make it difficult to form a fist, grasp small objects, or perform other manual tasks. In chronic and/or untreated cases, the muscles at the base of the thumb may waste away. Some people are unable to tell between hot and cold by touch.

Diagnosis of carpal tunnel syndrome is based on the history of symptoms, presence of risk factors, physical and neurological examination, and diagnostic tests.
Neurological examination includes testing the muscle that abducts the thumb away from the palm (called the abductor pollicis brevis), as well as the ability to bend the thumb toward the palm (flexion) and ability to move the thumb toward the other fingers (opposition). Tinel’s sign (tapping the palm sharply produces tingling) and Phalen’s sign (pressing the backs of the hands together for about 1 minute produces pain and numbness) are also evaluated.
Nerve conduction velocity (NCV) and electromyography (EMG) are used to evaluate nerve and muscle function. NCV involves placing electrodes on the skin above the median nerve to monitor the speed at which an impulse travels along the nerve. EMG involves placing small electrodes into the abductor pollicis brevis muscle to detect abnormalities that may indicate that the median nerve supplying the muscle is damaged. These tests, which are often referred to as EMG/NCV studies, may reveal delayed nerve conduction in the median nerve.
Differential diagnosis includes inflammation (radiculopathy) of nerve roots C6 and C7 in the cervical spine and compression of the median nerve outside the carpal tunnel.
Treatment for carpal tunnel syndrome involves activity modification and rest, splinting, medication (including injection therapy), and surgery.
Activity Modification. The first line of treatment usually involves resting the wrist and avoiding activity and movement that worsen symptoms. The wrist may be immobilized using a removable splint. For most patients, wearing the splint at night relieves symptoms, and for others, wearing the splint while at work helps.
When the condition is work related, a work-site evaluation may be performed. An occupational therapist, physical therapist, or rehabilitation consultant is often able to suggest modifications to relieve the condition. Wrist and body positioning can often be improved using ergonomics (science used to fit a job to a person’s anatomy and physiology). Improving body position, stretching periodically, and changing positions frequently may help alleviate symptoms.
Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs; e.g., ibuprofen [Advil®, Motrin®]) may be used to relieve pain. Due to potentially severe gastrointestinal and cardiovascular side effects, NSAIDs should only be used as instructed.
Cortisone (a corticosteroid) may be injected into the area around the carpal tunnel to reduce inflammation and nerve compression. Lidocaine (a local anesthetic) may be combined with cortisone, or injected alone, to relieve pain. Lidocaine combined with cortisone produces longer-lasting pain relief.
Surgery often provides permanent relief of symptoms when other treatment measures fail.
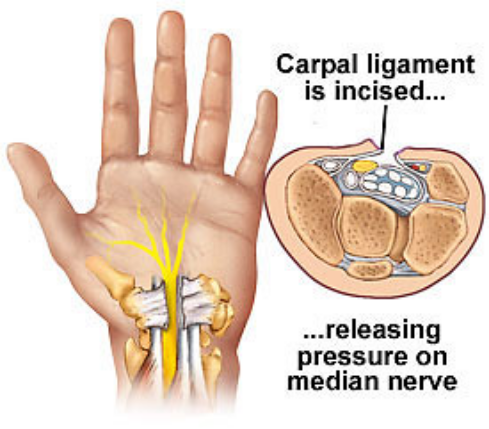
Carpal tunnel release involves cutting the transverse carpal ligament to relieve entrapment of the median nerve. It is usually performed on an outpatient basis, using local, regional, or general anesthesia.
Carpal tunnel release can be performed as open or endoscopic surgery. In open surgery, an incision is made through underlying tissue in the palm of the hand to reach the carpal ligament.
In endoscopic surgery, a smaller incision is made in the wrist and an endoscope is used to locate the carpal ligament. Surgical instruments are inserted through the incision or through a small incision in the palm and the ligament is cut.
Recovery usually takes 3 to 12 months. If compression has caused permanent nerve damage, carpal tunnel release surgery may not be effective.
Complications associated with the surgery include the following:
. Adverse reaction to anesthesia
. Burning pain caused by nerve damage (causalgia)
. Incomplete release of the ligament (more common in endoscopic surgery; requires additional surgery)
. Infection
. Nerve damage (rare)
. Stiffness
. Swelling
Laceration of a nerve, blood vessel, or tendon is more common in the endoscopic procedure and this approach is not recommended for patients who have small wrists.
Prognosis. Nonsurgical and surgical treatment for carpal tunnel syndrome relieves symptoms in approximately 90% of cases.
Prevention. Maintaining proper posture, body position, and technique when performing repetitive wrist movements may help to prevent carpal tunnel syndrome. It is important to relax, move around, and change positions frequently when performing any one task for an extended period of time.
The ReBuilder’s patented electrical signal has been proven 94% effective in clinical studies in reducing or eliminating symptoms of neuropathy.


Contact Us
Newsletter
Quick Links
Contact Info
Frequency Rising
13239 Sundance Ave. San Diego, CA 92129
800-701-4039 9am – 5pm PST
info@peripheralneuropathytreatments.com